The Hyperventilation Syndrome – Dr. Frances Ames Part II
CHAPTER 3 - CLINICAL SYMPTOMS AND SIGNS
This series comprises forty patients who were seen during a two-year period at Groote Schuur Hospital. They were referred for investigation from wards or out-patient departments. Most of them came from the neuro-psychiatric or medical departments. Two came from surgical wards.
Ten cases were hospitalized because of the hyperventilation syndrome (though not diagnosed as such on admission); five cases manifested symptoms and signs of the syndrome while in hospital for other complaints, and twenty-five cases were referred to the out-patient departments with a variety of diagnoses.
AGE
The oldest patient was 54 years, the youngest 17. The average age was 30.9 years.
- Under 20 years 10 patients
- 20 - 29 years 7 patients
- 30 - 39 years 12 patients
- 40 - 49 years 8 patients
- 50 years and over - 3 patients
SEX
27 females, 13 males.
RACE
35 Europeans. 4 Coloured. 1 Malay. Clinically almost all systems of the body were involved. Symptoms and signs are described and discussed under each separate system.
RESPIRATORY SYMPTOMS AND SIGNS
Symptoms
Twenty-four patients complained of respiratory difficulty, but in only one of them was it the main complaint. Many did not mention it unless asked directly. Only three patients realized that they were overbreathing. The characteristic description of the respiratory difficulty was, "I could get air into my chest but felt unsatisfied", or, "I felt that I could not get a deep enough breath". Associated with this sensation there was often a feeling of being shut in or oppressed. Patients complained that the chest felt "tight" and they felt that they must get fresh air. In some cases this led to extraordinary behavior: one man drove through town holding the door of his car open, "to let in all the air"; a woman always rushed out of her house, whatever the hour, if she got an attack, "because I felt I would die for lack of air"; another patient tore open his collar "to let all the air in".
Two patients complained of "panting for breath" during attacks. One complained that she yawned excessively and when a hyperventilation test was done on her she began to yawn uncontrollably after 30 seconds.
Two patients complained that they got a stuffy feeling in the nose at the onset of an attack and were forced to breathe through the mouth. During hyperventilation tests, the majority of the subjects automatically breathed through the mouth.
Previous "respiratory conditioning" was seen in three patients; one of them said, "My wife is asthmatic and watching her struggling for breath makes me feel that I can't get enough air"; another woman said, “my attacks started just after my child died from a gland bursting in her throat and suffocating her"; a third said, “I have a congenital heart and doctors are always asking me about my breathing".
The respiratory difficulty might come on at any time but occurred most frequently when the subject was tired or upset, in a crowded place, or preparing for sleep. Five subjects were awakened from sleep by respiratory difficulty and occasionally the marriage partner would awaken the heavily breathing subject "before an attack developed".
The characteristic and striking feature of the respiratory difficulty was that it was never related to exertion. If it appeared to be so related, questioning always revealed that it occurred either after or before - never during exertion. Indeed, in some cases, it was actually relieved by some form of physical activity and many patients said, “When I got the trouble with breathing I was restless and had to walk up and down, and that seemed to help me".
The patient in whom the respiratory difficulty was the chief complaint was a man of 45 years, who said that three or four times a week during the previous year he had been getting, attacks when he "could not get a proper breath". This woke him from sleep and he would jump out of bed contorting his body grotesquely in search of respiratory satisfaction. Sweat poured off him, his abdomen became distended and he felt giddy. Attacks lasted about 30 minutes.
Fifteen patients denied any respiratory difficulty.
Interestingly enough seven of these had gross hyperventilation attacks while under observation in hospital. Even at this time, they denied any breathing difficulty. An eighth was instructed to overbreathe and promptly developed one of her "fits". Her mother, who was watching the procedure, said, "Oh, she always breathes like that during an attack but I did not think it important enough to mention in the history".
Two patients said that they did not notice anything wrong with the breathing, "but my friends always know when I am going to get an attack because my breathing gets so deep.”
No independent evidence was available of the breathing during attacks of the remaining five patients in this series.
Goldman (1922) claimed that a person must double his respiratory volume before becoming conscious of his breathing. McCance (1932) reports two cases where "scarcely noticeable overbreathing tetany was induced.”
Signs
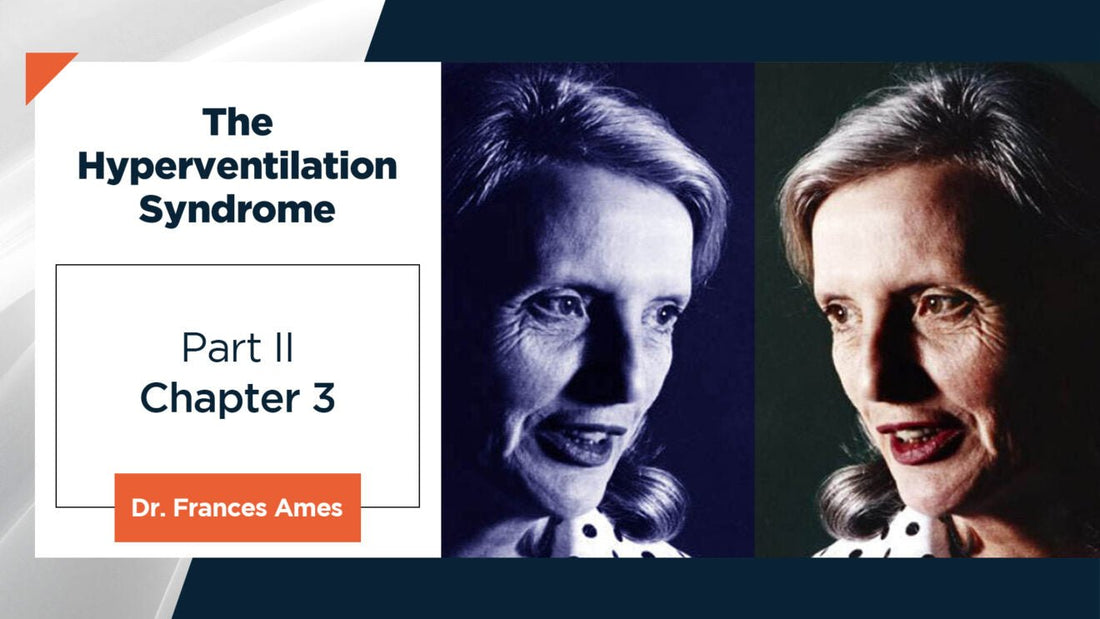
Chronic irregularity of breathing was found in two of ten patients of whom respiratory tracings were taken (Fig. 1 (a) and (b)).
Hyperventilation took the form of:
- Deep, fairly rapid breathing. This was the common type. Subjects usually opened their mouths at this time.
- Very fast, shallow breathing or panting. This was seen in only two cases. It should be noted that when patients were told to "pant" their breathing was still usually deeper than normal.
(Type of breathing after hyperventilation - See Experimental section, page 53).
Pathogenesis
Within a few seconds of overbreathing, the alveolar CO2 tension drops from the normal of 40 mmHg to 15-20 mmHg. It does not diminish much further despite continued overbreathing. The resulting alkalemia is responsible for many of the clinical manifestations.
CEREBRAL SYMPTOMS AND SIGNS
Symptoms
Thirty-one patients complained of some cerebral disturbance. Twenty-six of them described it as one of several complaints. Where peripheral complaints were prominent, cerebral complaints received cursory mention. The most common complaint was giddiness, faintness, or lightheadedness - never a true vertigo. This sensation was always aggravated by the upright posture and relieved by recumbency. It was often accompanied by blurring of vision or "black spots before the eyes''. Patients were usually afraid of falling and were unsteady on their feet: one man seldom ventured out of his house because, if he had to cross a busy street, his "hands and feet would tingle and he would become so giddy that he was afraid he would fall"; one woman refused to climb stairs because of her lightheadedness. “A tight band around the head", or actual headache, was sometimes complained of. Some patients said they felt as if they were drunk and staggered and one woman who had a hyperventilation attack on a bus was actually threatened by the conductor with a charge of drunkenness.
Several patients complained of "a feeling of unreality" as though they were not quite in touch with their surroundings. A doctor once described to me a seance which he attended in company with a young girl who had recently been bereaved. He said: “In the darkness, I could hear her breathing heavily. Suddenly she screamed and as the lights were switched on and a pencil thrust into her hand she scrawled DAD with tetanic fingers. The girl, because of the strange feeling of unreality, was quite sure she had been in touch with the spirit of her dead father".
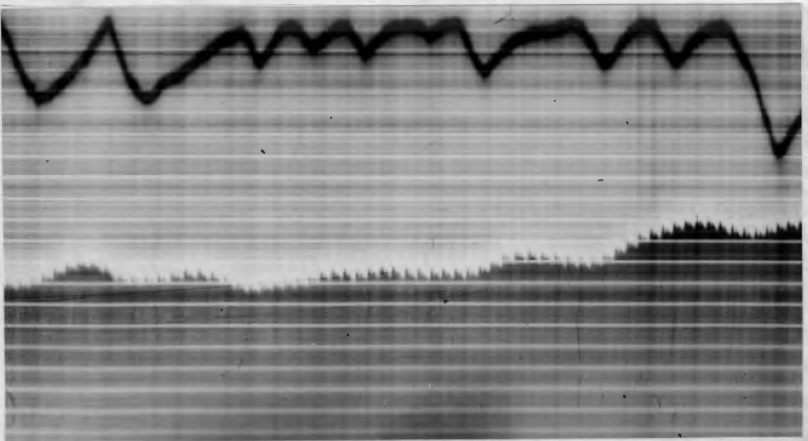
Fig. 1 (a) - Respiratory tracing and plethysmogram of a hyperventilator. This is the "normal" breathing pattern of this patient. Notice the gross irregularity, including involuntary deep breaths. Also, note the small pulse volume.
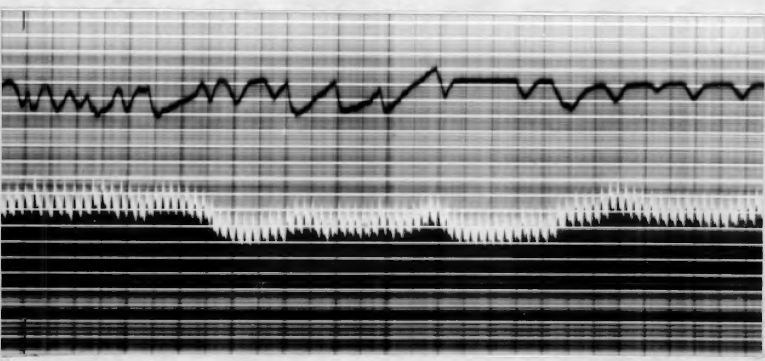
Fig. 1 (b) - Respiratory tracing and plethysmogram of a normal subject when emotionally disturbed. Note that an irregularity of breathing similar to that shown in fig. 1 (a) is present.
Drowsiness - often associated with yawning - was often seen after a hyperventilation test of 2 - 5 minutes. One woman always hyperventilated herself to sleep.
Loss of inhibition is common. Several patients wept or laughed during attacks. For this reason, a hyperventilation test can sometimes be used as a simple abreaction technique.
One patient presented with abnormal behavior as her chief complaint. Her story was that she had been worried for some months about her chest. One morning she had to run to catch a train. She was breathless as she got in and became alarmed at her “bad chest". For the next 20 minutes, she sat on the train with a feeling of "not being able to get a deep enough breath". As the train drew into the station she felt so peculiar that hardly knowing what she was doing, she wrenched open the door of the moving train and fell heavily onto the platform. A hyperventilation test reproduced this "peculiar feeling" so exactly that she attempted to get up and run out of the room.
The term "blackout" was not infrequently used by patients. This almost always turned out to be a sense of giddiness with a fear of falling but no actual loss of consciousness. Only five patients in this series had a disturbance of consciousness gross enough to merit the term "blackout". (See Appendix-cases 14, 16, 17, 24, 26)
It is interesting that of the nine patients who had no cerebral symptoms always had their hyperventilation attacks when in bed. The recumbent posture diminished cerebral symptoms.
Signs
The disturbance of consciousness can be well illustrated by getting the patient to do a task involving a fair degree of coordination, or to solve an arithmetical problem, immediately after several minutes of overbreathing.
Pathogenesis of the Cerebral Symptoms
The cerebral symptoms point to some definite but easily reversible change in brain activity. This is supported by the fact that there is usually a correlation between disturbance of consciousness and electroencephalographic changes during hyperventilation. Certain of these changes are regarded as indicative of epilepsy.
Four types of EEG change may occur
- The most common is the appearance of a high voltage slow rhythm of 2 to 3 cycles per second - the so-called delta rhythm. (See fig.2). The factors which determine the appearance of delta activity are not completely understood. Brazier, Finesinger, and Schwab (1944) working with young adults found that 38% of "normals" developed delta activity. All workers agree that delta activity results ultimately from acapnia but they do not agree about the immediate cause. Three possibilities have been suggested - (Hill and Parr, 1950).
(a) Inadequate compensatory vasoconstriction (Gibbs, Lennox and Nims, 1942).
(b) Cerebral anemia due to vasoconstriction resulting in anoxia and glucose deprivation (Davis and Wallace, 1942).
(c) Reduction in the activity of the cholinergic supply to the blood vessels of the cortex resulting in excessive local constriction (Darrov, and Pathman, 1943-44).
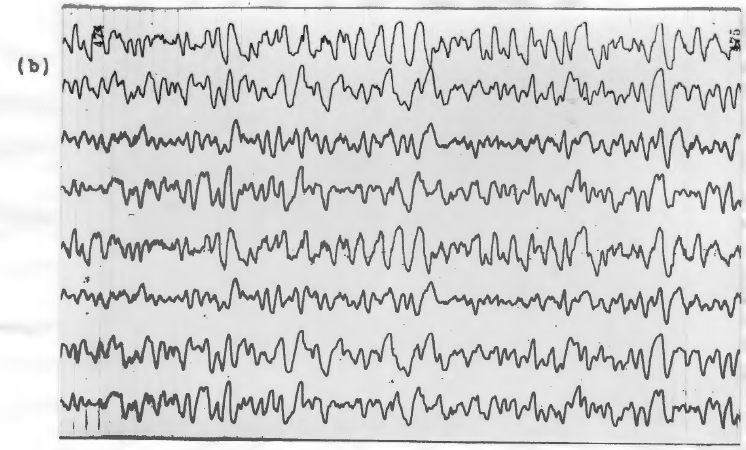
Fig. 2. Electroencephalogram of a subject (a) before 2 minutes of hyperventilation (b) after 2 minutes of hyperventilation. Note the appearance of large delta waves in (b).
It has been suggested that a reasonable working hypothesis is "to regard the delta activity as resulting from a failure of oxidative metabolism in the brain cells and in particular of the oxidation of glucose since the instability may often be prevented by raising the 02 and glucose levels in the blood". (Hill and Parr, 1950).
It is not unusual, however, for delta activity to appear with no clearly detectable change in consciousness and apparently some subjects can become unconscious during hyperventilation and yet show no delta activity.
- The resting alpha rhythm may increase in amplitude without becoming faster than the normal 8-14 cycles per second.
- Abnormally fast rhythms may appear or fast rhythms already present may increase in amplitude. If an already existing fast rhythm doubles in voltage or a fast rhythm appears, especially if it appears in bursts, the present tendency is to classify the phenomenon as epileptic.
- Both fast and slow rhythms may appear in the well-known spike and wave pattern. This is almost certainly diagnostic of epilepsy. It usually occurs in young patients with petit mal.
These EEG changes disappear within a few seconds when the subject stops overbreathing. It seems that the loss of CO2 is the fundamental factor. The cerebral circulation is very sensitive to chemical changes in the blood and it is generally accepted that the fall in the CO2 content of the blood as a result of overbreathing causes the cerebral blood vessels to constrict, thus both reducing the blood flow and conserving CO2 in the brain. Kety and Schmidt (1946), using the nitrous oxide method, measured changes in cerebral blood flow in five volunteers during active and passive hyperventilation. They found that cerebral blood flow invariably diminished - the mean decrease being 33% during active hyperventilation and 35 percent during passive hyperventilation. The cerebral arteriovenous O2 difference invariably increased (average 58%) and the cerebral O2 consumption showed a consistent and significant increase during active hyperventilation (average 15%) but no change during passive hyperventilation.
PERIPHERAL NEUROLOGICAL SYMPTOMS AND SIGNS
Thirty-three patients complained of these.
Sensory symptoms
Sensory symptoms occur earlier than motor. They appear at a variable time after the onset of overbreathing, depending on the rate and depth of breathing and the susceptibility of the subject. Some patients have marked symptoms after two or three deep breaths and others may overbreathe for 5 or more minutes before getting symptoms. The symptoms consist of paresthesia variously described as "tingling", "pins and needles”, "electric shock", “deadness" or "numbness". They always start distally. The usual pattern of spread is first in the fingertips and very often first in the ulnar area; then in the toes and finally in the peri-oral area and tip of the nose. Any one of these sites may be first or solely involved, depending on individual susceptibility. One extremity is frequently involved before the other and it is not necessarily the dominant one; one woman always got her paresthesia in the left hand and around the left side of her face and left ear. She said that her left ear also got deaf during attacks. She was quite sure that this was a form or “stroke". She was right-handed.
Finally, there may be a generalized tingling. Two patients complained that their teeth were tingling.
A feeling of spasm or tightness in the muscles or the extremities or midline structures, such as the epigastrium or sternum, is a common complaint.
Objective sensory loss then develops in the affected areas. Touch and later pain sensation are interfered with.
Motor manifestations
Motor manifestations consist of fascicular twitching which first involves the race and small muscles of the hands. It may appear spontaneously or be elicited by tapping near a peripheral nerve (Chvostek’s sign). Actual tetanic spasm was complained of by six patients - two of whom were alkalotic because of vomiting. If hyperventilation is continued the characteristic spasm of hands and feet develops. On the hand, this consists of adduction and extension of the thumb with extension of the interphalangeal and flexion of the metacarpophalangeal joints. Finally, flexion of the wrist occurs. In the feet the ankles are inverted, tarsus flexed and toes extended. In the face the eyes have a staring look due to contraction or the orbicularis oculi, the jaw is clenched and the corners of the mouth drawn up.
Patients often complain of difficulty in articulation because of "stiffness" of the mouth. The larynx may be involved with the production of stridor.
One patient complained of laryngeal stridor, which is uncommon in adults. She was a European female of 52 years who said that four years previously she had had a thyroidectomy. At this operation, her recurrent laryngeal nerve was cut. One month after the operation she was recognized as being myxoedematous. Eight months after the operation she had an attack of stridor. After this, she often woken herself and her family at night by stridor. Her serum calcium is normal. During the day she sometimes got a tingling in her hand and a feeling of "not being able to get a deep enough breath".
Spasm of hands and feet may be painful. It can be relaxed voluntarily, despite continued hyperventilation, if the spasm is not too well established. In one subject who demonstrated this, there was a lag or a few seconds before the hand reverted to its tetanic posture.
Proximal muscles are later involved and if the spread of the spasm is mainly unilateral there may be some diagnostic difficulty: one woman always got tingling in the left hand with drawing up of the left shoulder; the possibility of a Jacksonian attack was considered in her case but the whole picture was reproduced many times by hyperventilation tests.
Muscles or trunk and head area are later involved with the development of opisthotonus. Three cases (not included in this series) were sent to the hospital diagnosed as meningitis because of this marked opisthotonus end neck rigidity. Within a few minutes of cessation of overbreathing, the neck rigidity disappeared and the head assumed its normal position.
The involvement of trunk muscles may be associated with abdominal pain and rigidity. This presented a diagnostic puzzle in two surgical cases. They were both patients with partial intestinal obstruction who had been vomiting and so were in a state of alkalosis. They became alarmed about themselves and began to overbreathe. Tetanic spasm developed and later rigidity of abdominal muscles. The question of perforation then arose but once they had stopped overbreathing the rigidity disappeared.
Marked muscle tenderness may be present in limbs previously the site of tetanic spasm. A nurse was sitting talking to her friends when she developed tingling in her hands and feet. She then collapsed with tetanic spasms in the extremities. After a night of hyperventilation tetany, her muscles were so tender and "weak" that she was sent into hospital as a case of poliomyelitis.
Hemi-tetany is very uncommon. Patients often start with paresthesia in one limb but by the time tetanic spasm has been supervened they have generalized symptoms and signs. If, however, there has been some organic nervous disease, especially hemiplegia, hyperventilation may result in hemi-tetany. One such case was a European male of 38 years who one month before hospital admission had developed left-sided hemiplegia due possibly to a vascular accident. His signs cleared up so that clinically there was only minimal evidence of hemiplegia. One morning he woke with his left hand in tetanic spasm. Then he became conscious of a tingling feeling on the left side of his mouth and his left leg became stiff. "I did not think I was overbreathing but my wife says I was breathing deeply". The attack passed off in 15 minutes and he had many such attacks before hospital admission. A hyperventilation test was carried on for 30 minutes. He developed well-marked tetany on the left side with minimal paresthesia on the right. Plethysmography showed no difference in the pulses on the left and right sides.
Pathogenesis
Kugelberg (1946 and 1948) claimed that tetanic activation was ultimately dependent on peripheral nerve change. The pattern of spread was always the same in that the long tactile fibers to the face and hands were first activated, which caused the sensation of tingling. Later other afferents were activated - giving rise to the sensation of spasm. Then the longest motor fibers to the small muscles of the hand were excited (extensors having a lower threshold than flexors). Finally, the shorter fibers to flexor carpi ulnaris were affected.
Kugelberg has done electromyographic studies to show not only the same distinctive type of response but also a distinctive spread of response in all varieties of tetany. He emphasized the primary involvement of the nerves to face and hands and pointed out that these were the parts best represented in the cerebral cortex and most recent phylogenetically. He suggested that the difference in vulnerability of the various nerve fibers might be due to the size of the fiber or to the state of calcium in the fiber.
ALIMENTARY SYMPTOMS AND SIGNS
Symptoms
Many patients complained of dryness or the mouth which was probably due to overbreathing through the mouth.
One patient complained of a bitter taste in the mouth; another of a fishy taste.
Eight patients complained of abdominal distension during an attack. This was usually relieved by belching.
Two patients complained of epigastric discomfort. One of them said, “During the attack, my stomach feels as though it has turned to jelly". Another complained of a "vice-like" feeling across the epigastrium.
One patient in this series complained of nausea, and it was complained of by one normal control after a 2-minute overbreathing test.
Signs
Rigidity of abdominal muscles may be striking during an attack of hyperventilation tetany.
Pathogenesis
Air swallowing has been suggested as one possible mechanism for the distension. (See fig. 3).
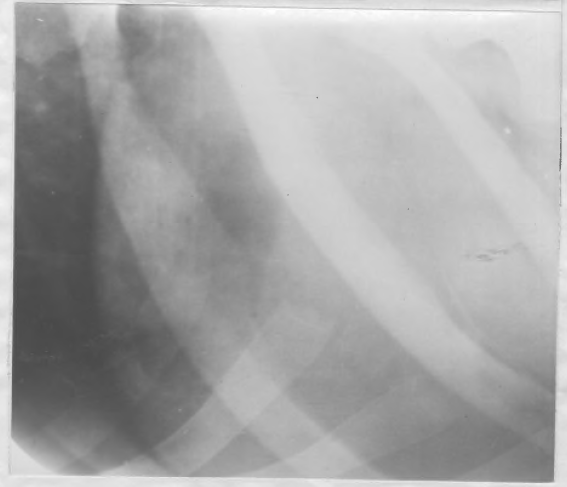
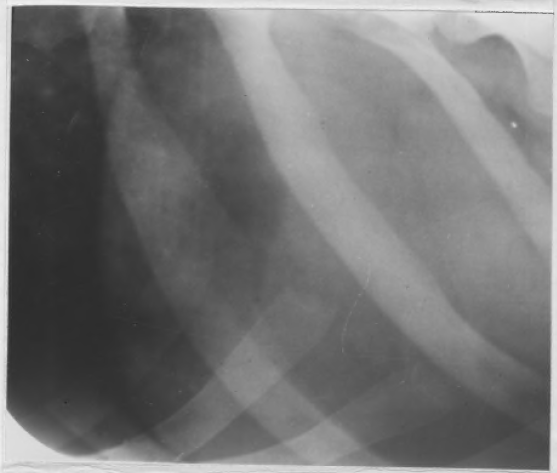
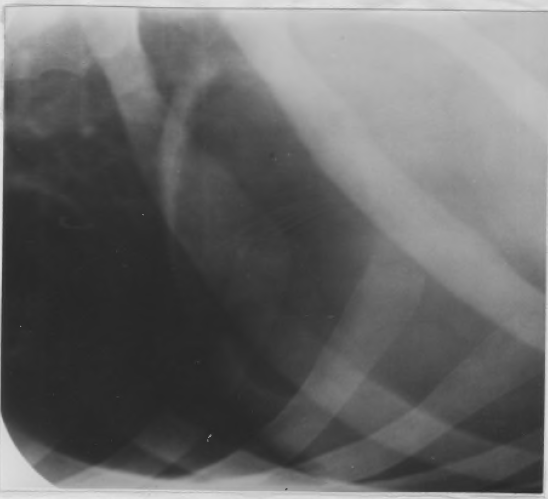
Fig. 3. (a) (b) (c) X-ray of the stomach (a) before, (b) immediately after, and (c) 10 minutes after 5 minutes overbreathing in a normal subject. Note the increase in the amount of intragastric air after overbreathing. The time of exposure and development was constant for all three x-rays.
Another explanation for apparent gross distension is a marked increase in lumbar lordosis. (Westdahl 1951, Roussak 1951). This was seen in a Malay a.man who always became drastically "distended" during hyperventilation. Her back was round to be arched several inches off the couch and she refused to relax it saying that it would aggravate her breathing difficulty if she did so.
A tight feeling and rigidity of abdominal muscles are due to increased neuromuscular excitability.
SYSTEMIC CIRCULATORY SYMPTOMS AND SIGNS
Symptoms
Eight patients complained of precordial pain. In one case the pain had all the characteristics of angina but was apparently never provoked by any form of exercise other than hyperventilation. One woman got a "burning" feeling under the sternum after a few minutes of overbreathing. Another patient complained of "a sharp pain under the breast bone which shoots up to my left shoulder and around my neck". Two patients complained of an oppressive feeling in the left precordium "as though something is pressing on my heart." Another patient complained of a "dull ache" over the left precordium. Two patients said they got a sharp stabbing pain "like a knife" in the left mammary region.
Ten patients complained of palpitations. In one case it was the sole complaint.
Six patients complained of cold hands and feet, but in only one was it the main complaint. Several patients, after several minutes of overbreathing, complained of a generalized coldness and shivered violently.
Peripheral vasoconstriction was a striking feature in all cases after a few minutes of overbreathing. The hands and feet became cold and sweated freely. Two cases became cyanosed. In some cases, the radial pulse was obliterated. An increase in pulse rate from 6 to 30 beats per minute occurred. In all cases after a few minutes of overbreathing. (See experimental section).
Pathogenesis
Precordial pain of the knife-like or aching left mammary variety might result from the misuse of the respiratory musculature. Any departure from the normal smooth action of breathing might cause fatigue of intercostal muscles or the diaphragm. Wood (1941) invoked diaphragmatic spasm as a cause of the precordial pain seen in Da Costa's syndrome.
The "pressing pain around the heart" was relieved in both cases by belching so that distension of the stomach caused by air swallowing might account for this form of discomfort.
Cardiospasm was thought to be responsible for precordial pain in two cases.
Pain that simulates coronary artery disease has led to serious diagnostic errors. Electrocardiographic changes also occur during overbreathing so that the problem may become very difficult. The changes consist of lowering of the S-T segment and lowering or inversion of T waves. There are various theories to account for these changes. Some workers invoke anoxia of heart muscle or coronary vasoconstriction. Others put them down to changes in the position of the heart or associate them with the tachycardia that occurs.
It can be argued that overbreathing is a form of exercise so that true angina could be precipitated by a hyperventilation test. It is also true that some patients with undoubted coronary artery disease hyperventilate through fear and anxiety. Several patients (outside the present series) with definite evidence of coronary occlusion described paresthesia in the limbs as part of the attack. In these cases, careful history taking revealed that the patients had been overbreathing.
Tachycardia is partly explained by the muscular exercise of overbreathing.
The peripheral vasoconstriction that occurs in hyperventilation is dealt with in the experimental section, page 49.
Urinary Symptoms and Signs
Urinary changes which have been reported after overbreathing are alkalinity of the urine, the presence of bicarbonate but little or no ammonia, diuresis, and slight ketonuria.
In this series, two patients complained of diuresis after overbreathing. In six normal controls, the urine became alkaline and showed an increase in phosphates after 8-10 minutes of overbreathing.
Pathogenesis
Some of the urinary changes result from the alkalosis. It is possible that the diminution in cerebral blood flow may partly account for the diuresis or the phosphaturia through a pituitary or hypothalamic mechanism.
The phosphaturia is interesting because, according to Brown and Hilton (1930), it is "noted most frequently in association with wasting, worry, serious mental depression or severe mental work or strain".
GENERAL SYMPTOMS AND SIGNS
Fatigue is a common complaint after a hyperventilation test.
Pathogenesis
Hyperventilation is a vigorous form of physical exercise.
COMMENT ON CLINICAL EFFECTS OF HYPERVENTILATION
It is characteristic of the hyperventilation syndrome that, despite its wide and varying pattern of symptoms and signs, the nervous system is always involved. Every case in this series had some evidence of neurogenic dysfunction. Engel, Ferris, and Logan (1947) suggested that patients could be classified according to whether this neurogenic dysfunction was mainly cerebral or mainly peripheral. A grouping of the patients in the present series in this way gives:- mainly cerebral involvement, seven cases; mainly peripheral neurological involvement, nine cases; both cerebral and peripheral, twenty-four cases.
Individual patterns of reaction tend to remain stable in different subjects: a subject whose first symptom is a tingling in the left ulnar region will always tend to start with that symptom.
The pattern is, however, sometimes upset. Among the factors which seem to disturb it are:
(a) Posture. The upright posture aggravates cerebral symptoms.
(b) Low blood sugar level. This also aggravates cerebral symptoms. Engel et al. (1947) quoted a case of a woman who always reacted to overbreathing with cerebral symptoms if she was starving and with tetany, if she had just had a high carbohydrate meal.
(c) Unknown factors. A few subjects vary in their reaction patterns for no apparent reason. A medical man who often acted as a subject in these experiments would on one day manifest tetanic spasm, on another day, cerebral symptoms and yet on other occasions, laryngeal stridor would be an early and striking manifestation.
The time of onset and the severity of symptoms and signs vary both from subject to subject and at different times in the same subject. Some subjects get severe symptoms so quickly after starting to hyperventilate that as a clinical observation they can be classed as hypersensitive. There is at present, however, no satisfactory scientific measure of this hypersensitivity. O'Donovan (1943) defined a hypersensitive person as one who developed tetany within 2 minutes of overbreathing at the rate of 55- 60 breaths per minute, or who was so incapacitated by the severity of the symptoms that hyperventilation could not be carried on for longer than 2 minutes. This does not take into account depth of breathing, or the fact that subjects with a large vital capacity may blow off their CO2 more rapidly. It also ignores the subjective factor that a person who is tired or feeling demoralized may very quickly feel that his symptoms are too severe to enable him to carry on. Many patients in this series where the breathing rate used were 40 breaths per minute complained that "they could not carry on" when asked to overbreathe for 2 or 3 minutes. Some refused to continue for more than a few seconds. Yet they could not be called hypersensitive to overbreathing in any measurable physiological sense.
Individual sensitivity does not necessarily make one a sufferer from the hyperventilation syndrome, though one is more likely to develop dramatic symptoms if one does overbreathing. Only three subjects, using tetany production within 2 - 3 minutes of overbreathing at the rate of 40 breaths per minute as the criterion for hypersensitivity, could be classed as abnormally sensitive. Two of these were not patients but "normal controls".
Variation in the time of onset and the severity of symptoms in the same subject at different times seemed to be due to fatigue or stress, or both. Patients often remarked that although the symptoms produced in a hyperventilation test were essentially the same as those produced during involuntary overbreathing in response to stress, they were less severe. The physiological and biochemical changes produced in the body during stress lie outside the scope of this thesis. Mention must be made, however, of one factor which may play a part in enhancing the effect or symptoms directly attributable to overbreathing. This factor is that of adrenaline release. Adrenaline is a well-recognized respiratory stimulant; it may be involved in initiating or sustaining the overbreathing. Further, by its action in causing vasoconstriction of skin vessels, adrenaline enhances the reflex peripheral vasoconstriction of overbreathing.
The effect of adrenaline in precipitating tetany in subjects rendered alkalotic by overbreathing has been sporadically investigated for many years. In 1925 Duzar and Hensch claimed that if normal children overbreathed for 5 or 6 minutes they could be made actively tetanic by intravenous adrenaline, without further hyperpnoea. McCance (1932) thought that the only effect of adrenaline administration in aggravating hyperventilation tetany was its action as a respiratory stimulant. Harvey and Lilienthal (1942) found that intraarterial injection of adrenaline in hypocalcemic patients precipitated tetanic spasm. They thought that this was due to the “abrupt distortion of the potassium-calcium ratio” which occurs after adrenaline administration and not to the intense vasospasm that also occurred, or to any change in breathing rate. They investigated one subject suffering from the hyperventilation syndrome and reported that adrenaline, without preliminary hyperpnoea, did not precipitate tetanic spasm. But their final comment on this case appears significant: “after the test, he began moderate, voluntary hyperventilation and induced well-marked carpopedal and facial tetany within one minute“.





