The Hyperventilation Syndrome - Dr. Frances Ames Part V
Download in pdf-format >>
TABLE l. The changes in pulse volume after a single deep breath in normal subjects and in hyperventilators.
| Normal subjects. | Normal pulse volume ml. | Pulse volume after 1 deep breath ml. | Duration of change in pulse volume. sec. | Normal respiratory rate. Breath/min. | Normal pulse rate. Beats/min. |
| L. | 0.018 | 0.01 | 25 | 18 | 78 |
| D. | 0.012 | 0.007 | 20 | 24 | 72 |
| M. | 0.021 | 0.011 | 43 | 21 | 78 |
| A. | 0.012 | 0.006 | 25 | 12 | 72 |
| P. | 0.008 | 0.004 | 20 | 18 | 90 |
| S. | 0.025 | 0.012 | 60 | 24 | 72 |
| WC. | 0.013 | 0.005 | 20 | 20 | 72 |
| C. | 0.012 | 0.004 | 30 | 24 | 72 |
| AVERAGE | 0.0151 | 0.0073 | 30.3 | 20.1 | 75.7 |
| Hyperventilators | Normal pulse volume ml. | Pulse volume after 1 deep breath ml. | Duration of change in pulse volume. sec. | Normal respiratory rate. Breath/min. | Normal pulse rate. Beats/min. |
| Wi. | 0.006 | 0.003 | 25 | 21 | 78 |
| A. | 0.005 | 0.002 | 20 | 21 | 78 |
| K. | 0.01 | 0.005 | 12 | 18 | 78 |
| B. | 0.01 | 0.005 | 20 | 18 | 90 |
| H. | 0.005 | 0.003 | 20 | 24 | 78 |
| R. | 0.01 | 0.002 | 30 | 24 | 84 |
| M. | 0.011 | 0.005 | 35 | 18 | 66 |
| N. | 0.01 | 0.005 | 30 | 18 | 72 |
| AVERAGE | 0.0083 | 0.0037 | 24 | 20.2 | 78 |
Comment
A reflex exists whose afferent path is not precisely known. The stimuli that trigger it are: the act of taking a breath of sufficient depth; the act of making an obstructed respiratory effort (where the movement of the chest is nearly as great as that in taking a deep breath); and a series of rapid, shallow breaths. The different path is by way of the sympathetic nerve fibers. The response is vasoconstriction which reduces peripheral pulse volume to less than half of its initial height and reduces the rate of arterial inflow. This peripheral vasoconstriction persists for an average of 30 seconds.
In normals and in hyperventilators the reflex vasoconstriction after a deep breath has the same characteristics. The only striking difference between the two groups is that the average hyperventilator has generally a smaller pulse volume than the normal subject so that any procedure that produces vasoconstriction causes a considerable reduction in peripheral blood flow.
2. The effect of 2 minutes of overbreathing
The time period of 2 minutes was chosen because previous experience had shown that some of the subjects developed tetanic spasms if they hyperventilated for longer. This broke the seal of the plethysmograph and interrupted the experiment.
Subjects were instructed to breathe deeply at a rate of 30 to 40 breaths per minute. A metronome was tried initially to regulate the rate exactly but was later abandoned because it introduced the factor of mental activity. The depth was not regulated because to achieve this too complicated a procedure is required.
The same subjects were used as those in the first series of experiments.
The table shows the results obtained and the graph illustrates some of the points. (Table 2, Fig. 15).
The normal controls finished their 2 minutes of hyperventilation with:
(a) An average pulse volume of 0.0051 ml.
(b) A persistence of this vasoconstriction for an average of 3.2 minutes.
(c) An average pulse rate of 95 beats per minute.
(d) A respiratory tracing that in six of eight cases was notable for periods of apnoea of several seconds duration.
(e) A persistence of the abnormal respiratory rhythm for an average of 2.8 minutes.
The hyperventilators finished their 2 minutes of overbreathing with:
(a) An average pulse volume of 0.0039 ml.
(b) A persistence of this vasoconstriction for an average of 5.7 minutes.
(c) An average pulse rate of 97 beats per minute.
(d) A respiratory tracing that in only one case showed any evidence of apnoea and in some cases showed an increase in depth compared with the breathing before hyperventilation.
(e) A persistence of the respiratory abnormality for an average of 3.7 minutes.
The hyperventilators after 2 minutes of overbreathing have a smaller peripheral blood flow than the normal controls. In addition, this vasoconstriction persists much longer. The interpretation of the pathogenesis of the vasoconstriction after 2 minutes of overbreathing is more complicated than that following a single deep breath.
Table 2
The changes in pulse volume after 2 minutes of overbreathing in normal subjects and in hyperventilators
| NORMAL CONTROLS | L. | D. | M. | A. | P. | S. | Wc. | C. | AVERAGE |
| Pulse volume | 0.005 ml | 0.006ml | 0.005ml | 0.004ml | 0.002m | 0.01ml | 0.005ml | 0.006ml | 0.0051 |
| Pulse rate | 102 | 90 | 105 | 108 | 105 | 84 | 90 | 78 | 95.2 |
| Respiratory rate and character | 21 with no apnoeic periods | 12 with many apnoeic periods | 18 with apnoeic periods | 21 with apnoeic periods | 20 with apnoeic periods | 18 with numerous periods of apnoea | 14 with numerous periods of apnoea | 20 with periods of apnoea | 18 with 7 out of 8 showing apnoea |
| Persistence of respiratory abnormality | 4 mins | 2 mins | 2.5 mins | 3 mins | 3 mins | 2.5 mins | 2.5 mins | 3 mins | 2.8 mins |
| Persistence of vasoconstriction | 4 mins | 3 mins | 4 mins | 3 mins | 4 mins | 1.5 mins | 3.5 mins | 3 mins | 3.2mins |
| HYPERVENTILATORS | Wi. | A. | K. | BX. | H. | R. | M. | N. | |
| Pulse volume | 0.004ml | 0.0018ml | 0.003ml | 0.004ml | 0.003ml | 0.005ml | 0.005ml | 0.004ml | 0.009ml |
| Pulse rate | 96 | 120 | 102 | 108 | 96 | 90 | 78 | 90 | 97.5 |
| Respiratory rate and character | 15 with apnoeic periods | 24-no apnoea | 15 with apnoeic periods | 17-no apnoea | 30-no apnoea | 27-no apnoea, grossly irregular | 24-no apnoea | 24-no apnoea | 23 with 2 out of 8 showing apnoea |
| Persistence of respiratory abnormality | 2.5mins | 3.5 mins | 4 mins | 3 mins | 7 mins | 4 mins | 3 mins | 3 mins | 3.7mins |
| Persistence of vasoconstriction | 4 mins | 5.5 mins | 8 mins | 6.5mins | 10 mins | 3 mins | 6 mins | 3 mins | 5.7 mins |

Fig. 15. This illustrates the change in pulse rate and pulse volume of a normal control and a hyperventilator after 2 minutes of overbreathing. Note the small initial pulse volume and the persistence of vasoconstriction in the hyperventilator.
Two factors complicate the results:
1. A circulatory factor, manifesting itself in tachycardia. Presumably, this results from the physical exertion of overbreathing.
In both the normal controls and the hyperventilators this increase varied between 6 and 30 beats per minute and persisted in both groups for about 1 minute. It cannot, therefore, be invoked to explain any difference between the two groups as far as the degree and persistence of vasoconstriction are concerned.
It is, however, interesting to compare the response of a sympathectomized patient to the effects of the 2 minutes of overbreathing.
In this type of case, the reflex vasoconstriction in response to deep breathing does not occur because its motor path has been removed. A diminution in pulse volume nevertheless does occur and is correlated with the tachycardia. (Fig. 16 and 17).
2. The type of respiration after a period of hyperventilation is important.
Six of the normal controls showed a slowing of respiration due to many apnoeic pauses. (Fig.18).
This abnormality persisted for 2 to 3 minutes. The remaining two normal controls immediately resumed normal breathing but at a slightly slower rate.
Four of the hyperventilators continued to breathe much more deeply than before hyperventilation. (Fig. 19).

Fig. 16. Plethysmogram of the left big toe of a patient who had had a lumbar sympathectomy several months before this experiment. One minute of hyperventilation is illustrated. Note that a diminution in pulse volume occurs. This is due to the tachycardia.

Fig. 17. This shows the correlation between change in digital pulse volume and change in pulse rate after 2 minutes of overbreathing in a patient in whom the sympathetic chain had been completely removed.
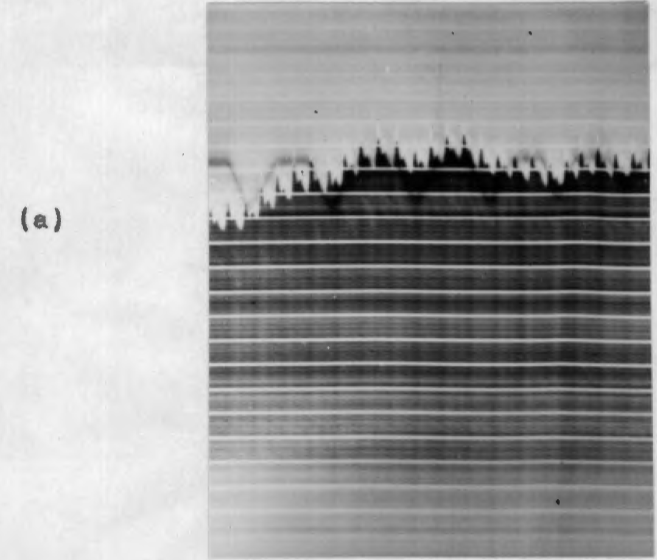
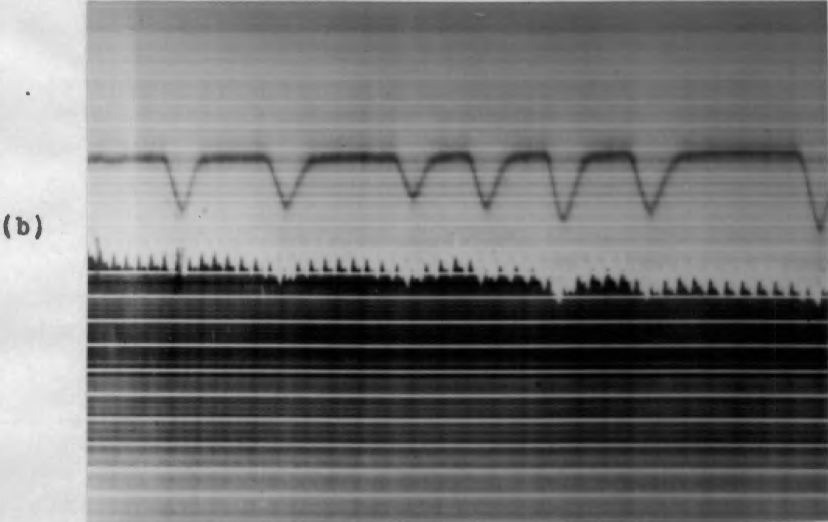
Fig. 18 (a) and (b). - Respiratory tracing of a normal subject -
(a) before 2 minutes of hyperventilation.
(b) and after 2 minutes of hyperventilation.
Note apnoeic periods in (b).
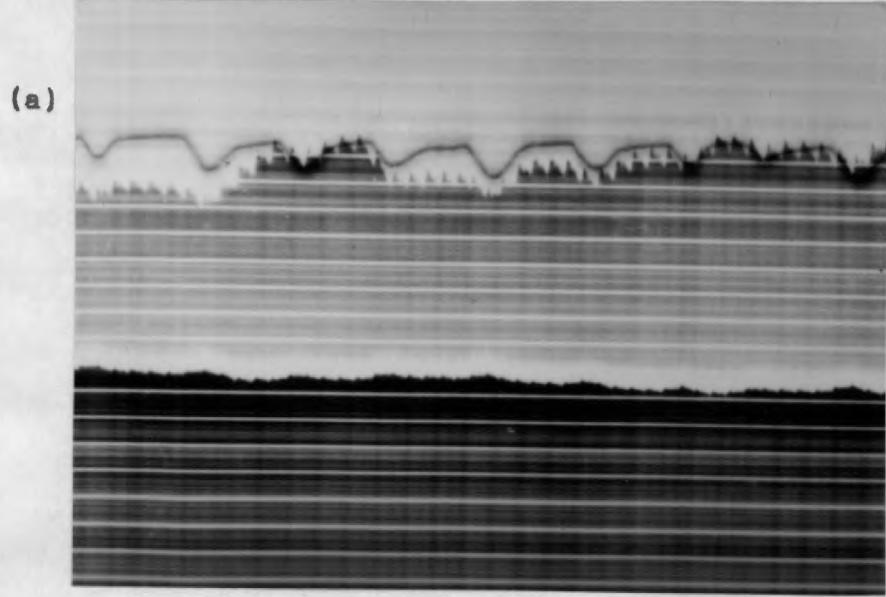
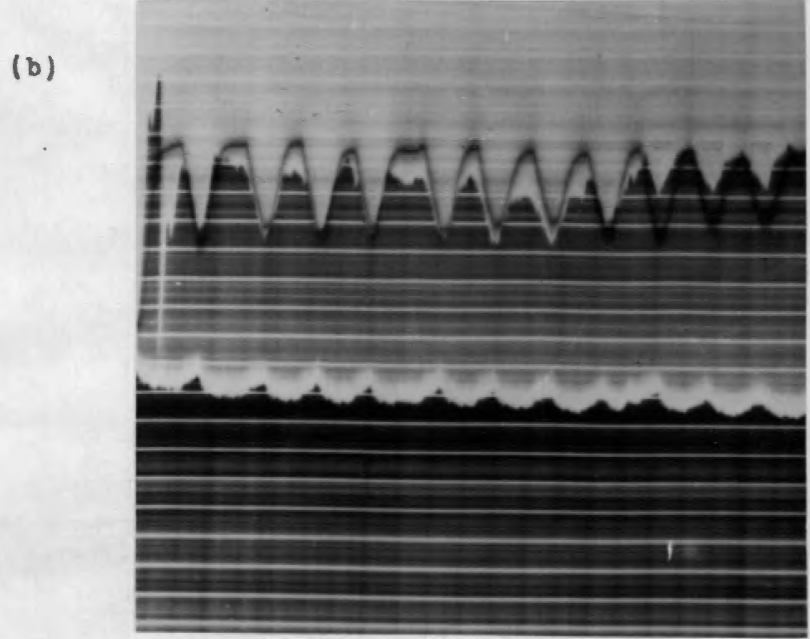
Fig. 19 (a) and (b). Respiratory tracing in a hyperventilator -
(a) before 2 minutes of hyperventilation and
(b) after 2 minutes of hyperventilation.
One patient showed grossly irregular respiration with many periodic deep breaths and spells of rapid, shallow breathing.
Two patients resumed normal breathing but at a slightly slower rate.
Only one patient showed any apnoea and he spontaneously remarked that he had consciously held his breath after the experiment because the whole mechanism of hyperventilation with its consequent physiological changes had been previously explained to him.
The respiratory abnormality in the hyperventilators persisted for 3 to 4 minutes.
It is obvious that the first five hyperventilators would tend to remain in a state of vasoconstriction longer than the normal controls by virtue of the increased depth of their breathing, or periodic deep breaths.
The remaining three patients had, however, no respiratory cause for a lengthy persistence of vasoconstriction after hyperventilation. Two of these cases had a vasoconstriction that lasted 6 and 8 minutes respectively. This may be due to a more rigid vasomotor tone than in normal subjects.
3. The effect of hyperventilation:
(a) In ten normal controls with one hand warm and the other cool.
(b) In ten normal controls with the limbs elevated.
(c) In two patients at varying intervals after a two-stage sympathectomy of the upper limbs.
(a) Ten normal controls free of any organic vascular disease were used for this experiment.
Both hands were simultaneously immersed in water - one hand at a temperature of 57°F and the other at a temperature of 110°F. If the water is made too hot or too cold the subjects experienced discomfort in the hands which interfered with their accurate observation of the paraesthesia resulting from hyperventilation.
The hands were immersed for 1 1/2 minutes. They were then dried by the experimenter. The subject was then seated comfortably with the hands resting lightly on a table. Care was taken to ensure that there was no pressure on peripheral nerves. The subject then began to hyperventilate at a rate of about 35 breaths per minute. The time and place in which paresthesia manifested themselves were noted. The experiment was repeated the following day with the hands interchanged. (Table 3).
It was found that if the experiment was repeated too soon - that is some hours later - the hand in which paresthesia had been most intense during the first experiment always tingled first in the second experiment. It appears that the irritability of the peripheral nerve induced by overbreathing may persist for a considerable time - certainly several hours.
TABLE 3. Times of onset of paresthesia in ten subjects who e.re instructed to hyperventilate with one hand cooled and the other warmed. The hand that was initially cooled is put first.
Subject Cold hand Results during hyperventilation
| I. | (i) Left | After 2 minutes left hand began tingling. After 5 minutes no tingling in the right hand but cerebral discomfort so marked that the experiment was stopped. |
| (ii) Right | After 2 minutes right hand began tingling. After 4 minutes no tingling in the left hand. | |
| V. | (i) Right | After 4 minutes right hand began tingling. After 5 minutes left hand began tingling. |
| (ii) Left | After 3 minutes left hand began tingling. After 4 minutes right hand began tingling. | |
| L. | (i) Right | After 2 minutes right hand began tingling. After 3 ½ minutes, the left hand began tingling. |
| (ii) Left | After 2 minutes left hand began tingling. After 5 minutes no tingling in the right hand. | |
| S. | (i) Left | After 1 minute left hand began tingling. After 3 1/2 minutes, the right hand began tingling. |
| (ii) Right | After 2 minutes right hand began tingling. After 3 minutes left hand began tingling. | |
| M. | (i) Right | After 1 1/2 minutes, the right hand began tingling. After 2 1/2 minutes left hand began tingling. |
| (ii) Left | After 1 1/2 minutes left hand began tingling. After 2 ½ minutes, the right hand began tingling. | |
| D. | (i) Left | After 3 minutes left hand began tingling. After 3 1/2 minutes, the right hand began tingling. |
| (ii) Right | After 4 minutes right hand began tingling. After 5 minutes left hand began tingling. | |
| A. | (i) Right | After 2 minutes right hand began tingling. After 2 1/2 minutes left hand began tingling. |
| (ii) Left | After 1 1/2 minutes left hand began tingling. After 2 minutes right hand began tingling. | |
| M. | (i) Left | Bilateral tingling more intense in the left hand. |
| (ii) Right | Bilateral tingling equally intense in both hands. | |
| L. | (i) Left | After 2 minutes left hand began tingling. After 3 ½ minutes, the right hand began tingling. |
| (ii) Right | After 2 minutes left hand began tingling. After 3 minutes right hand began tingling. | |
| W. | (i) Left | After 1 minute right hand began tingling. After 2 minutes left hand began tingling. |
| (ii) Right | After 2 minutes right hand began tingling. After 3 minutes left hand began tingling. |
From Table 3 it can be seen that in seven of the ten subjects hyperventilation resulted in paraesthesia in the cold hand first - whether that hand was the right or the left. In one subject the temperature of the hands did not seem to make any difference as he developed paresthesia simultaneously in both the cold and warm hand, after overbreathing for a few minutes. In one subject paresthesia always appeared first in the left hand, whether it, was warm or cool. In one subject paresthesia always appeared first in the right hand whether it was warm or cool.
Comment
It seems therefore that in most people local cooling of a hand will hasten the appearance in that hand of the paraesthesia resulting from overbreathing.
Two of the subjects were right and left-handed dominant as far as the onset of paresthesia was concerned. The point has already been mentioned in the clinical section that in some people the site of the initial tingling is always the same. This local susceptibility does not seem to depend on any vascular factor and it is apparently strong enough to overrule any temperature differences.
(b) The effect of hyperventilation in elevated limbs.
Ten normal controls free of any organic vascular disease were used for this experiment. The subject lay on the floor with the head on a pillow. One leg was extended and the other elevated at an angle of about 75 degrees. The heel rested against the side of a padded couch. One arm was supported by the observer without compressing any peripheral nerves. The other arm was extended at the side of the subject. This posture was maintained for 2 minutes to accustom the subject to it. The subject then began to overbreathe and reported on the development of paresthesia.
TABLE 4. Times of onset of paresthesia in ten subjects who were instructed to hyperventilate while one leg and one arm were kept elevated.
Subject Limb Elevated Results during hyperventilation
| L | L. leg | After 1 minute tingling began in the left leg. |
| R. arm | After 2 minutes tingling began in the right arm. After 4 minutes tingling began in the right leg. | |
| S. | L. leg | After 5 minutes tingling began in the left leg. |
| R. arm | After 6 minutes tingling began in the right arm. | |
| D. | L. leg | After 1 minute tingling began in the left leg. |
| R. arm | After 3 minutes no tingling anywhere else. Cerebral symptoms so marked that refused to continue overbreathing. | |
| W. | L. leg | After 2 minutes tingling began in the left leg. |
| R. arm | After 4 minutes tingling began in the right arm. | |
| V. | R. leg | After 3 minutes tingling began in the right leg. |
| L. arm | After 4 minutes tingling began in the left leg. | |
| M. | R. leg | After 2 minutes tingling began in the right leg. After 3 minutes tingling began in the left leg. |
| L. arm | After 3 1/2 minutes tingling began in the left arm. After 5 minutes tingling began in the right arm. | |
| LO. | R. leg | After 3 minutes tingling both hands. No paresthesia in feet. |
| L. arm | After 5 minutes too uncomfortable to continue. | |
| A. | L. leg | After 3 minutes tingling began in the left leg. |
| R. arm | Subject too uncomfortable to continue overbreathing. | |
| T. | R. leg | After 2 minutes tingling began in the right arm. |
| L. arm | After 3 minutes tingling began in the right leg. Subject too uncomfortable to continue overbreathing. | |
| M. | R. leg | After 2 minutes tingling began in the right leg. |
| L. arm | After 3 minutes tingling began in both hands. After 4 minutes tingling began in the left leg. |
From Table 4 it can be seen that in eight subjects paresthesia first became manifest in the elevated leg; in one subject in both hands; and in one subject in the non-elevated arm. In no subject did the elevated arm tingle first though in three cases it took second place to the elevated leg. Four subjects were unable to complete the experiment despite their recumbent attitude. They found the unnatural position of the limbs too trying when allied with the usual unpleasant symptoms of hyperventilation.
Comment
Elevation of the leg hastens the onset of the paraesthesia resulting from hyperventilation. This is remarkable because normally with the subject recumbent the legs are often late in manifesting paresthesia.
(c) The effect of hyperventilation in two patients at varying intervals after a two-stage sympathectomy of the upper limbs.
This patient was a European female of 20 years who suffered from acrocyanosis. She was an excellent witness. The experiment was performed 5, 7, 13, and 24 days after the right arm had been adequately sympathectomized.
(i) After 5 days:
The right arm was warm and dry, the left cold and blue.
The patient lay recumbent and began to overbreathe at about 35 breaths per minute. She was told to report any unusual sensations immediately. She reported as follows:
- After 2 minutes: tingling in right hand;
- 3 minutes: coldness in left hand;
- 4 minutes: the whole right arm tingling markedly;
- 5 minutes: jaw tingling;
- 10 minutes: tingling started in left hand;
- 15 minutes: right arm felt numb and "dead".
- 25 minutes: subjective stiffness of the right hand and adduction of the thumb - commencing tetanic spasm. At this time there was only slight tingling in the left hand.
Throughout the experiment, the right hand remained warm and dry while the left hand became progressively colder and sweated profusely.
(ii) After 7 days:
The experiment was repeated. The patient reported:
- After 2 minutes: dizziness;
- 3 minutes: tingling in right hand;
- 4 minutes: tingling in legs;
- 6 minutes: slight tingling in the left hand. (At this stage the patient began to yawn uncontrollably and continued to do so till the end of the experiment.)
- 9 minutes: a lame, tingling feeling in the whole of the right arm and still slight tingling in the left hand;
- 15 minutes: tingling increased in left hand;
- 17 minutes: tetanic spasm commenced in the right hand.
(Throughout the experiment the right hand remained warm and dry while the left hand became progressively colder and sweated profusely).
(iii) After 13 days (and 5 days after the left arm had been sympathectomized): at this time both 60. hands were warm and dry. The patient had some slight tingling in the left ulnar distribution, probably the result of traction on the brachial plexus during the second operation.
She reported:
- After 1 minute: dizziness;
- 3 minutes: both hands tingling;
- 5 minutes: both legs tingling;
- 6 minutes: uncontrollable yawning;
- 7 minutes: her whole body twitching;
- 12 minutes: continued to yawn and felt sleepy.
- 13 minutes: the whole of left arm tingle much more markedly than the right side;
- 16 minutes: left arm felt "very funny - sort of lame and tingly".
- 20 minutes: left arm still tingled markedly, a little tingling of the right hand.
(iv) After 24 days (and 17 days after the left arm had been sympathectomized): at this time both hands 1ere warm and dry and the slight tingling in the ulnar distribution had diminished. The patient breathed at 40 breaths per minute - reasonably deeply.
She reported:
- After 3 minutes: dizziness;
- 4 minutes: pain in chest;
- 5 minutes: slight tingling in both hands - more intense in left ulnar nerve distribution;
- 10 minutes: generalized shivering and feet felt very cold;
- 11 minutes: slight tingling in both forearms;
- 16 minutes: both legs tingling;
- 18 minutes: both arms felt "dead";
- 26 minutes: both arms tingling and legs felt "dead";
- 28 minutes: hands and feet tingling markedly and fingers "stiff";
- 44 minutes: tingling sensation wore off in hands, except in the left ulnar nerve area, legs still tingling slightly and feet cold and sweating, face and ears tingling markedly. She remarked that the tingling was much less than on previous occasions. There was no motor spasm throughout the experiment.
Comment:
The first two tests were carried out 5 days and 7 days after the right arm had been sympathectomized. Twenty minutes of overbreathing resulted in the appearance of tetanic spasm in the right hand with moderate paresthesia in the left hand.
The third test was carried out 13 days after the right and 6 days after the left arm had been sympathectomized. On this occasion, the left hand developed marked paresthesia with minimal tingling in the right hand.
The fourth test was carried out 24 days after the right and 17 days after the left arm had been sympathectomized. On this occasion paresthesia of moderate-intensity developed in both hands. This wore off later despite continued hyperventilation and never progressed to tetanic spasm.
In other words, the subject with an established sympathectomy was much less susceptible to the manifestations of peripheral nerve irritability resulting from hyperventilation than is a normal subject. Forty-four minutes of reasonably vigorous hyperventilation in a normal subject will almost certainly produce a well-marked tetanic spasm in the arms.
The transient increase in susceptibility of the sympathectomized limbs a few days after the operation could be explained by postulating a temporary irritability of the peripheral nerves as a result of traction on the brachial plexus at operation. This does occur and did so in this case because the patient had symptoms of left ulnar nerve irritation.
2. This was a European female of 28 years who was suffering from acrocyanosis.
(i) The first experiment was done preoperatively. The patient was very apprehensive. She reported as follows:
- After 1 minute of overbreathing: markedly dizzy;
- 3 minutes: felt cold (her whole body began to shiver);
- 7 minutes: tingling in both hands - much more intense on the left side.
She refused to continue hyperventilation.
Her hands at the onset of the experiment had been blue and cold and became progressively colder and sweated profusely.
(ii) Experiment is repeated 11 days after the left arm had been sympathectomized. She did not have Horner’s syndrome. The left hand was warm and dry and the right cold and blue.
She began to hyperventilate at 36 breaths per minute and flexed her legs because she could "breathe better".
- After 2 minutes: giddiness;
- 5 minutes: Tingling began in right hand;
- 6 minutes: her teeth began chattering but she said she was not very cold;
- 11 minutes: "lameness" in the left hand - but no tingling;
- 14 minutes: right hand tingling markedly;
- 16 minutes: feet began to tingle;
- 21 minutes: right arm and both feet tingling markedly;
- 24 minutes: right hand stiff and felt "terrible".
- 26 minutes: tetanic spasm right hand. At this time the left hand felt normal apart from slight "lameness".
20 days after the left arm had been sympathectomized and 6 days after the right arm had been sympathectomized:
- After 3 minutes: dizziness;
- 6 minutes: both feet tingling markedly;
- 7 minutes: generalized shivering;
- 9 minutes: slight laryngeal stridor;
- 11 minutes: marked stridor - became extremely anxious and semi-conscious with thrashing around of her limbs. The experiment was stopped.
Comment:
This woman differed from the previous patient in that the sympathectomy was not so extensive - she did not develop Horner's syndrome as the stellate was not completely removed.
Before her operation hyperventilation results in paraesthesia in both hands - more markers on the left side. Eleven days after the left arm had been sympathectomized 26 minutes of hyperventilation resulted in a tetanic spasm of the right hand and paresthesia in the legs. In the left hand, there was only slight “lameness".
Twenty days after the left arm had been sympathectomized and 6 days after the right arm had been sympathectomized 11 minutes of overbreathing resulted in paresthesia in both feet but no change in the hands. The laryngeal stridor terminated the experiment.
A comparison of her reactions before and after sympathectomy shows that the operation made her upper limbs less vulnerable to the peripheral nerve signs resulting from hyperventilation. She did not show the transient increase in susceptibility that the first case showed. This can be attributed to the fact that the operation, being less extensive, did not interfere with the brachial plexus.
Previous Chapter
Chapter 6 - Experimental Section
Next Chapter